

Occupational therapy’s role in LTC
I was visiting with my 90-year-old grandmother in her little apartment in an assisted living complex and asked her if she wanted to move to a long-term care (LTC) facility. I thought it would give her more access to activities and socialization. She looked at me and said, “Why? Do you want me to die?” Unfortunately, this is what many people think about long-term care.
When residents are admitted to LTC facilities, many show little interest in daily activities and even if some residents are able to bathe or dress themselves, they often report the staff does these tasks for them. Because I wanted to make a difference at the rural facility where I worked, I knew I needed to help others understand the positive effects occupational therapy (OT) can have on the health and quality of life for residents.
PROJECT RATIONALE
It is disheartening to see older adults giving up when they could continue to live fulfilling lives. Carlson, Clark and Young1 describe how elderly people can achieve life satisfaction when engaged in productive activities. They also found that aging with greater social connections leads to better health.
In another study,2 the authors found some participants in the study did not identify interests or initiate activities due to a loss of determination or a sign of reduced hope late in life. It is frustrating to see older adults act this way. “Occupational therapists have long held assumptions that the ability to engage in pleasurable occupations affects a person’s hope for the future.”2
In a 2008 research study,3 the authors developed a program of activities of daily living (ADLs) to increase physical activity and functional abilities for older adults in an LTC facility. When I thought about the LTC facilities I have seen, and my grandmother’s comment about these places being a place to die, I knew I wanted to make some changes.
When OTs work with residents, they typically assess their ADL skills to determine what they can do to assist the person to become proficient in ADL activities. I wanted other healthcare professionals to understand that OTs can continue to work with residents and look at the skills the resident has such as toileting, bathing, balance, range of motion, etc., but incorporate more about the resident and his or her background into the activity.
What if OTs and the other members of the interdisciplinary team entered a caregiving relationship based on the individualized needs and personal desires of residents? What if the OT found out more about the resident’s lifetime occupation or typical routines? Do they like to stay up late and sleep in late in the mornings? Do they have distinct preferences in food? Do they prefer to a bath or a shower? What about daily occupations? Do they like to watch television, read or socialize? What about their cognitive patterns, are they able to recall names of family members or friends, or do they remember significant dates in their lives?
As healthcare professionals, we must first understand each other’s roles and use the resources we have right in front of us. There is no doubt, any person who works in long-term care wants to enhance the quality of life for residents, but it cannot be accomplished alone. Healthcare professionals have traditionally been educated in isolation from one another, and do not understand the roles of the other professions.
Curran, et al4 conducted a mixed-method study to determine the effectiveness of using training modules for “enhancing collaborative competencies and fostering interprofessional collaboration in primary healthcare settings.” Training in this way can increase knowledge to the other professionals and enhance the care provided to the patients. If LTC administrators want to enhance the quality of life within a rural community by providing high-quality residential health services, it must be done collaboratively.
Occupational therapists help people participate in their lives through meaningful activities and help them to identify the types of activities that give them the most satisfaction. Successful aging is part of helping elderly people have more meaning in their lives. OTs’ goals are to promote health and well-being with individuals. To accomplish such goals, OTs provide treatments that are unique since they use activities to engage people and help them become self-sufficient. The stigma that life is over for someone in long-term care needs to be changed.
INTERVENTION PLAN
My desire to help others and to change the culture of a small upstate New York LTC facility led me to undertake an evidence-based occupational therapy (EBOT) project. I wanted to determine if healthcare professionalswho attended in-service trainings about the effects of OT interventions would increase their knowledge of OT’s role in enhancing the quality of life. A series of in-services were developed and implemented with healthcare professionals to find out. The in-service sessions included learning activities, discussions, Power Point presentations and interactive activities. Outcome evaluation measurements included pre/post in-service surveys as well as a focus group meeting to see how participants felt about the in-service sessions.
In addition, the in-service activities included simulated OT interventions typically done with LTC residents. Stations were set up for these simulated activities. One station, in particular, simulated a person with a visual impairment. After the simulations, it was explained what an OT would do when working with a person with visual disturbances. For example, I demonstrated the ways an individual without vision could safely navigate in certain environments. Interventions to prepare individuals with vision difficulties before ambulating were also demonstrated.
IN-SERVICE RESULTS
Results of the project were positive, because the healthcare professionals who participated increased their knowledge as to the roles of OTs in long-term care. 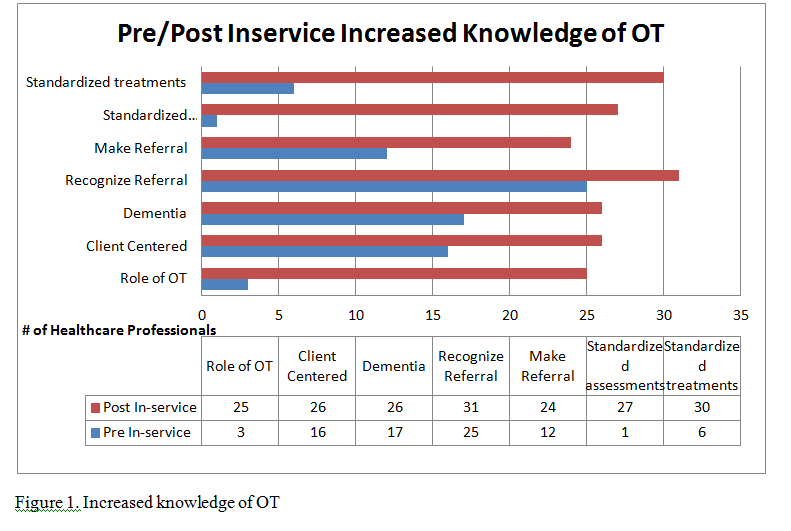 The increased knowledge was evident from the quantitative data that was gathered. Qualitative data was also gathered from the pre/post in-service surveys (see figure 1, right). The participants were asked to describe things they learned about OT because of the training(s).
The increased knowledge was evident from the quantitative data that was gathered. Qualitative data was also gathered from the pre/post in-service surveys (see figure 1, right). The participants were asked to describe things they learned about OT because of the training(s).
It is clear from the post in-service survey that healthcare professionals were able to understand OT can provide a variety of activities to help residents remain happy and lead fulfilling lives. The participant’s responses indicated 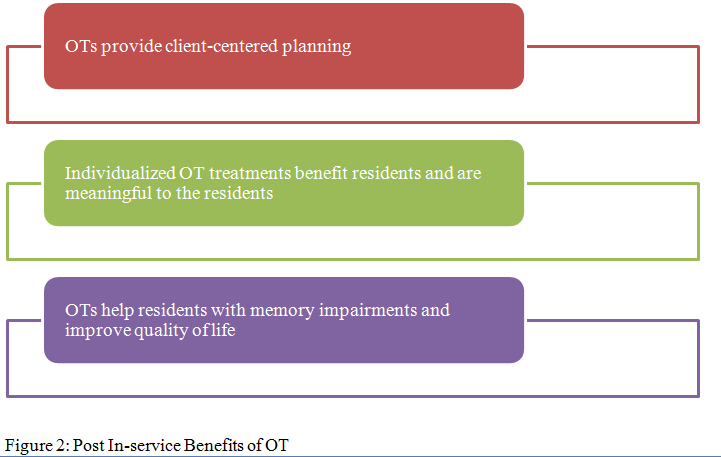 the increased knowledge from pre in-service surveys to post in-service surveys (see figure 2, left).
the increased knowledge from pre in-service surveys to post in-service surveys (see figure 2, left).
RECOMMENDATIONS
Several changes should occur in LTC settings to impact the quality of life of the residents more effectively. The work of this capstone project provides the foundation for future study and practice by OTs in LTC settings. The culture of these settings needs to continue to change and people need to in a homelike environment and exercise choice in what they want and like to do.
Michele A. Bennett, OTD, MSOTR/L, is an assistant professor of occupational therapy and an academic fieldwork coordinator at Keuka College, Keuka Park, N.Y. She has been a occupational therapist in New York since 2006. For more information, email mbennett1@keuka.edu.
REFERENCES
- Carlson M, Clark F, Young B. Practical contributions of occupational science to the art of successful aging: How to sculpt a meaningful life in older adulthood. Journal of Occupational Science 1998;5:107-18.
- Borrell L, Lilja M, Sviden, GA, Sadlo G.. Occupations and signs of reduced hope: An explorative study of older adults with functional impairments. American Journal of Occupational Therapy 2001;55(3):311-16.
- Peri K, Kerse N, Robinson E., Parsons, et al. Does functionally based activity make a difference to health status and mobility? A randomized controlled trial in residential care facilities (The Promoting Independent Living Study; PILS). Age and Ageing 2008;37:57-63.
- Curran V, Sargeant J, Hollett A. Evaluation of an interprofessional continuing professional development initiative in primary health care. Journal of Continuing Education in the Health Professions2007;27(4):241-52.
I Advance Senior Care is the industry-leading source for practical, in-depth, business-building, and resident care information for owners, executives, administrators, and directors of nursing at assisted living communities, skilled nursing facilities, post-acute facilities, and continuing care retirement communities. The I Advance Senior Care editorial team and industry experts provide market analysis, strategic direction, policy commentary, clinical best-practices, business management, and technology breakthroughs.
I Advance Senior Care is part of the Institute for the Advancement of Senior Care and published by Plain-English Health Care.
Related Articles








Topics: Activities , Alzheimer's/Dementia , Articles , MDS/RAI , Rehabilitation , Staffing